
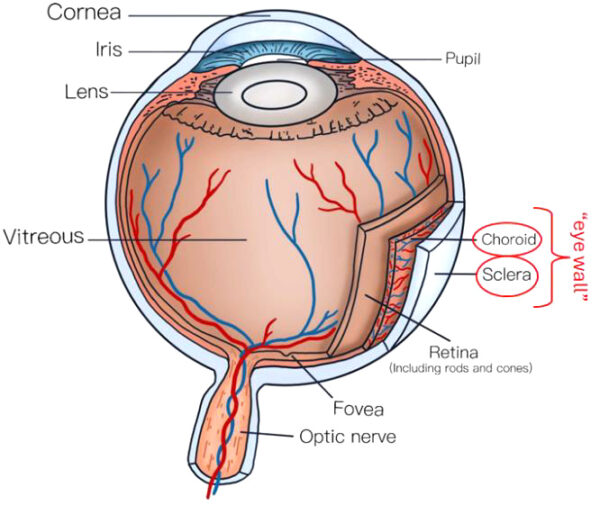
Myopia, or nearsightedness, is the most common form of refractive abnormality and is characterized by excessive eye elongation, causing distant objects to appear blurry. Elongation of the eye is further enabled by the thinning of the myopic “eye wall” – the choroid and the sclera as presented in Figure 1. Furthermore, with myopia, defocused light (DL) and longitudinal chromatic aberration (LCA) have been implicated as the probable mechanisms controlling eye growth. [1-5] Consequently, some of the proposed myopia control methodologies, like myopia-control lenses (D.I.M.S., H.A.L.T.), are based on these mechanisms. These myopia control lenses and others have been shown to have on average a 50 – 60% efficacy in stopping the progression of myopia, if worn for 10-12 hours daily and with the recommendation of 1-2 hours of outdoor activity while wearing myopia control lenses. [6-14] Figure 1. Schematic presentation of eye anatomy.
NeuroRays has noted that many pre-myopes and myopes have a retinal dopamine deficiency, thus implicating low retinal dopamine as a possible cause of myopia. This has been confirmed by reduced retinal activity measured by the b-wave amplitude of an electroretinogram. It is also known that low retinal dopamine can contribute to choroidal and scleral thinning, i.e. weak “eye wall”. [16]
Among other proposed solutions for myopia control, light therapies with different visible light wavelengths have emerged as promising and quick non-invasive solutions. [17-37] For instance, repeated low-level red light (RL) therapy has shown satisfactory results in stopping myopia progression with an efficacy rate of up-to ~90 %; however, rebound effects after the cessation of therapy have been observed. Other myopia control therapies, like injecting atropine or orthokeratology, have also shown rebound effects after their termination. [38-41] Knowing the mechanisms behind these myopia control therapies, especially those with rebound, might help find more efficient strategies for myopia control.
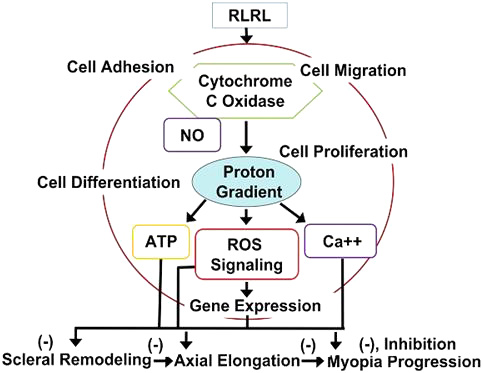
Several mechanisms have been proposed for the RL-based therapy for myopia control; the most accepted is the one via activation of the cytochrome oxidase (CCO) enzyme, as the primary photoreceptor of these long-range red wavelengths. CCO activation in fact improves retinal cell metabolism, reduces retinal inflammation and oxidative cell stress, all resulting in a better energy metabolism within mitochondria (Figure 2). Healthier retina and reinforced “eye wall” yielded the observed choroidal thickening and reduced axial length (AL) upon RL exposure. However, the rebound observed after stopping the RL therapy is most likely due to stopping of the energy/feed supply needed for maintaining a “healthy” mitochondrial metabolism. [17, 18]
Light therapies with exposure by shorter wavelengths (e.g. violet, blue, cyan) have also shown promising results – reduced AL, increased retinal and choroidal thickness and improved choroidal blood perfusion. Even in studies, when light defocus was not present, monochromatic blue light was the only light that showed reduced AL compared to the monochromatic green- and red-light exposures. [29] Therefore, blue light inhibits the development of myopia for reasons other than DL and LCA. To understand the mechanism behind the blue light exposure on myopia control, retinal dopamine and its role in the retinal-choroidal-scleral hierarchy (in the context of scleral hypoxia theory) needs to be explain first. The scleral hypoxia theory proposes that a weak choroid and reduced choroidal blood flow, leading to scleral hypoxia, plays a role in the development and progression of myopia. The oxygen deprivation in the sclera can trigger changes in the scleral extracellular matrix (scleral remodeling), potentially enabling further elongation of myopic eye, which will become even more myopic. [42-54]
Blue light (BL) exposure has been shown to generate retinal dopamine, a neurotransmitter, that prevents myopia progression in animal and human models. (Note: RL exposure has been shown to generate dopamine, as well, but to a much lower extent compared to BL). Blue light (or bright light) intensity and exposure time have been positively correlated with the retinal dopamine release. [42-50] A cascade of processes happens after a retinal dopamine release, which can further modulate the nitric oxide (NO) level in the retina. The relationship between retinal dopamine and NO is complex, with both neurotransmitters modulating the function of each other in the retina. For instance, NO can facilitate the release of dopamine, but with improper intensity and exposure may also block the re-uptake of dopamine, thus prolonging its effects. NO, as a vasodilator, increases the choroid blood flow, and thus, improves choroidal health and thickness. Better choroidal blood perfusion is a vital process for delivering oxygen and nutrients that nourish the outer retina (sclera), which improves the scleral health and stops its remodeling and thinning. Improved choroid and scleral health and thickness (reinforced “eye wall”) means better control over the ocular elongation – one of the main hallmarks of myopic eyes. It should be noted that increasing the amount of dopamine within the retina of an eye of a pre-myope or myope restores the proper activity level within the retina of the pre-myope or myope, while at the same time improving the health and strength of the eye’s sclera, both of which are believed to counter myopia. [51-54]
- Good blue light 480+/-30nm targets retinal rods and ipRGCs – increases Retinal Dopamine.
- Releases Nitric Oxide (a vasodilator) – promotes choroid blood flow – increases choroidal thickness and improves its health.
- Supplies Oxygen (O2) and Nutrients needed for scleral reinforcing – healthier sclera, which slows or stops myopia progression.

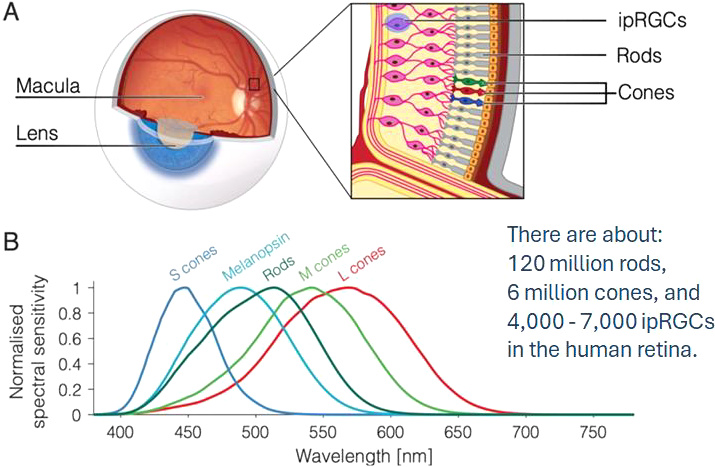
Furthermore, rods and melanopsin-containing intrinsically photosensitive retinal ganglion cells (ipRGCs) have been implicated in the generation of retinal dopamine after blue and cyan light exposure, ranging from 450 nm to around 510 nm. [55-57] Figure 4 is a schematic presentation of the eye with the three types of photoreceptors presented (A) along with their light sensitivities (B). While there is no available research data on potential rebound of BL effects on myopia control, NeuroRays believes that due to the major difference in the mechanisms behind the RL and BL, the rebound with BL treatment of myopia is less likely to occur.
In recent years, combination therapies for myopia control have been proposed with a potential to have higher efficacy in myopia control than the individual approaches. Synergistic effects have been observed when DIMS myopia control lenses are worn and only taken off during the RL therapy. In this case, an efficacy as high as 100 % has been reported. However, no data was reported regarding rebound potential. [58-72]
NeuroRays believes that BL therapy, combined with myopia control lenses (whereby the myopia control lenses are worn full time, and the BL therapy is applied through the myopia control lens to the eye), should provide the best outcome in terms of efficacy with little to no rebound. Estimated one or two short BL exposures (2-5 minutes per exposure) daily with myopia control glasses on, will have highly-efficient outcome – the blue light will be defocused and spread over the retinal periphery, where majority of rods, responsible for dopamine generation, are located. High levels of retinal dopamine are expected to be released starting the cascade of processes towards reinforcing the “eye wall” layers, the choroid and the sclera (Figure 3). The myopic eye with locked-in positive anatomical choroidal and scleral changes (due to the retinal dopamine release in conjunction with the continuous eyeglasses wear) will stop or significantly slow further myopia progression. The myope being treated with BL therapy may be able to stop the BL therapy (as long as they continue to wear their myopia control lenses) once the choroidal thickening occurs to a certain threshold level and the axial length has stopped its growth. It is believed that this method will cause the efficacy to quickly approach 100% and then with the assistance of the myopia control lenses there should be little to no rebound.
It is worth mentioning that with the ocular light therapy, maintaining retinal health (primarily that of the fovea and macula) has been a safety concern. For instance, with RL therapy, too much light intensity and exposure time to the fovea and macula can cause photo-thermal damage. Also, with BL therapy, the concern is that of phototoxicity of the fovea and macula, once again due to too much light intensity or time of exposure. (Note: Several studies with BL therapy have been done with BL wavelengths lower or around 450 nm, which is considered “bad blue light” with proven phototoxic effects on macula). NeuroRays has solved this potential safety problem by:
- Using good blue light (480+/-30 nm), which is safer than the “bad blue light”, and
- Utilizing a proprietary fixation target to cast a protective image over part or all of the macula. The fixation image can filter, block, or attenuate the amount of light intensity and exposure to the fovea and macula.
In summary, without question while myopia control lenses have proven to slow myopia progression, the efficacy has averaged between 50% – 60%. There is a need to improve this efficacy to be closer to 100%, while maintaining eye health and safety with little, if any, rebound. NeuroRays believes the following proprietary methodology can accomplish this goal:
- Ocular light therapy, utilizing fixation target-based macula protection, with exposure to eye(s) of 2 – 5 minutes per day “through” the myopia control lenses.
- Wear myopia control lenses daily and with time outdoors in the sun.
- When appropriate, stop the ocular light therapy, but continue to wear myopia control lenses daily indoors and outdoors for a period of time.
While RL therapy will work with the above approach, NeuroRays believes BL therapy will provide fewer rebound effects. Furthermore, with the above outlined proprietary approach and by using BL therapy there is a high likelihood of “safely” achieving close to 100% efficacy with little to no rebound.
US and Foreign Patents Pending
References
- National Academies of Sciences, Engineering, and Medicine, Myopia: Causes, Prevention, and Treatment of an Increasingly Common Disease. Washington, DC: National Academies Press. 2024, ISBN 978-0-309-71785-4
- Schaeffel, F. et al., Mechanisms of emmetropization and what might go wrong in myopia, Vision Research 220 (2024) 108402
- Erdinest, N. et al., Peripheral Defocus and Myopia Management: A Mini-Review, Korean J Ophthalmol 2023;37(1):70-81
- Delshad, S. et al, The human axial length and choroidal thickness responses to continuous and alternating episodes of myopic and hyperopic blur. PLoS ONE 2020, 15(12): e0243076.
- Biswas et al. The influence of the environment and lifestyle on myopia, Journal of Physiological Anthropology (2024) 43:7,
- Eppenberger, L. S. Myopia Control: Are We Ready for an Evidence Based Approach? Ophthalmol Ther (2024) 13:1453–1477
- Michaud, L. Myopia Management: Putting Theory in Practice, REVIEW OF OPTOMETRY, JUNE 15, 2024
- Liam, C. S. Y. et al., Long‑term myopia control effect and safety in children wearing DIMS spectacle lenses for 6 years, Scientific Reports, (2023) 13:5475
- Li, X. et al., Myopia control efficacy of spectacle lenses with highly aspherical lenslets: results of a 5‑year follow‑up study, Eye and Vision (2025) 12:10
- Bao, J. et al., Spectacle Lenses With Aspherical Lenslets for Myopia Control vs Single-Vision Spectacle Lenses, A Randomized Clinical Trial, JAMA Ophthalmol. 2022;140(5):472-478.
- Yuval, C. et al., Evaluating the Effect of a Myopia Control Spectacle Lens Among Children in Israel: 12-Month Results, Am. J. Ophthalmology, 2024, 257,103-112
- Arias, A. et al., In-depth optical characterization of spectacle lenses for myopia progression management, Optica, Vol. 10, No. 5, 2023
- Su, B. et al., A novel Lenslet-ARray-Integrated spectacle lenses for myopia control: a one-year randomized, double-masked, controlled trial, Ophthalmology (2024), 131 (12), 1389-1397
- He, X. et al., Time Outdoors in Reducing Myopia A School-Based Cluster Randomized Trial with Objective, Monitoring of Outdoor Time and Light Intensity, Ophthalmology 2022;129:1245-1254
- Chen, Y-Y. et al., The impact of light properties on ocular growth and myopia development, Taiwan J Ophthalmol 2024;14:143-150
- Schilling, T. et al., Increase in b-wave amplitude after light stimulation of the blind spot is positively correlated with the axial length of myopic Individuals, Scientific Reports, (2022) 12:4785
- Zhang, P. et al., Light Signaling and Myopia Development: A Review, Ophthalmol Ther (2022) 11:939–957
- Zhu, Q. et al., Repeated Low-Level Red-Light Therapy for Controlling Onset and Progression of Myopia-a Review, Int. J. Med. Sci. 2023, Vol. 20
- Liu, Y. et al., The effect of repeated low-level red-light therapy on myopia control and choroid. Transl Vis Sci Technol. 2024;13(10):29,
- Salzano, A.D. et al., Repeated Low-level Red-light Therapy: The Next Wave in Myopia Management? Optom Vis Sci 2023;100:812–822.
- Liu, Z. et al., The Effects of Repeated Low-Level Red-Light Therapy on the Structure and Vasculature of the Choroid and Retina in Children with Premyopia, Ophthalmol Ther (2024) 13:739–759
- Xiong, R. et al., Longitudinal Changes and Predictive Value of Choroidal Thickness for Myopia Control after Repeated Low-Level Red-Light Therapy, Ophthalmology 2023;130:286-296
- Xu, Y. et al., Repeated Low-Level Red Light Therapy for Myopia Control in High Myopia Children and Adolescents, Ophthalmology 2024;131:1314-1323
- Gu, L. et al., Axial Shortening Effects of Repeated Low-level Red-light Therapy in Children With High Myopia: A Multicenter Randomized Controlled Trial, Am. J. Ophthalmology, 2025, 270, p203-215
- Jiang, Y. et al., Effect of Repeated Low-Level Red-Light Therapy for Myopia Control in Children – A Multicenter Randomized Controlled Trial, Ophthalmology 2022;129:509-519.
- He, X. et al., Effect of Repeated Low-level Red Light on Myopia Prevention Among Children in China With Premyopia, A Randomized Clinical Trial, JAMA Network Open. 2023; 6(4):e239612.
- Dong, J. et al., Myopia Control Effect of Repeated Low-Level Red-Light Therapy in Chinese Children, A Randomized, Double-Blind, Controlled Clinical Trial, Ophthalmology 2023;130:198-204.
- Wang, X. et al., Effects of blue light exposure on ocular parameters and choroidal blood perfusion in Guinea pig, Experimental Eye Research 235 (2023) 109619
- Thakur, S. et al., Short-Term Exposure to Blue Light Shows an Inhibitory Effect on Axial Elongation in Human Eyes Independent of Defocus, IOVS | 2021 | Vol.62 | No.15 | Article 22
- Chakraborty, R. et al., Axial length reduction and choroidal thickening with short-term exposure to cyan light in human subjects, Ophthalmic Physiol Opt. 2024;00:1–19.
- Landis, E. G. et al., Ambient light regulates retinal dopamine signaling and myopia susceptibility. Invest Ophthalmol Vis Sci. 2021; 62(1):28.
- Landis, E. G. et al., Increased endogenous dopamine prevents myopia in mice, Experimental Eye Research, 193, 2020, 107956
- Chen, S. et al., Bright Light Suppresses Form-Deprivation Myopia Development With Activation of Dopamine D1 Receptor Signaling in the ON Pathway in Retina, Invest Ophthalmol Vis Sci. 2017; 58:2306–2316.
- Sarfare, S. et al., The effects of brief high intensity light on ocular growth in chicks developing myopia vary with time of day, Experimental Eye Research 195 (2020) 108039,
- Yuval, C. et al., Ambient illuminance, retinal dopamine release and refractive development in Chicks, Experimental Eye Research 103 (2012) 33-40
- Ashby, R.S. et al, The Effect of Bright Light on Lens Compensation in Chicks, Invest Ophthalmol Vis Sci. 2010; 51:5247–5253)
- Torii, H. et al., Violet Light Exposure Can Be a Preventive Strategy Against Myopia Progression, EBioMedicine 15 (2017) 210–219
- Bullimore, M. et al., Efficacy in myopia control – The impact of rebound, Ophthalmic Physiol Opt. 2024; 00:1–11.
- Xiong, R. et al., Sustained and rebound effect of repeated low-level red-light therapy on myopia control: A 2-year post-trial follow-up study, Clin Experiment Ophthalmol. 2022; 50:1013–1024.
- Chen, H. et al., Low-intensity red-light therapy in slowing myopic progression and the rebound effect after its cessation in Chinese children: a randomized controlled trial, Graefes Arch Clin Exp Ophthalmol. 2023; 261(2): 575-584.
- Chamberlain, P. et al., Eye growth and myopia progression following cessation of myopia control therapy with a dual-focus soft contact lens, Optom Vis Sci 2025;102: 353–358
- Zhou, X. et al., Dopamine Signaling and Myopia Development: What Are the Key Challenges, Prog Retin Eye Res. 2017; 61: 60–71.
- Landis, E. et al., Increased endogenous dopamine prevents myopia in mice, Exp Eye Res. 2020; 193: 107956.
- Landis, E.G. et al., Ambient light regulates retinal dopamine signaling and myopia susceptibility. Invest Ophthalmol Vis Sci. 2021;62(1):28.
- Carpena-Torres, C. et al., Increased ocular dopamine levels in rabbits after blue light stimulation of the optic nerve head, Experimental Eye Research 234 (2023) 109604
- Munteanu, T. et al., Light-dependent pathways for dopaminergic amacrine cell development and function, eLife 2018; 7:e39866.
- Brown, D. M. et al., Candidate pathways for retina to scleral signaling in refractive eye growth, Exp Eye Res. 2022; 219: 109071.
- Talwar, S. et al. Modulation of all-trans retinoic acid by light and dopamine in the murine eye. Invest Ophthalmol Vis Sci. 2025;66(3):37.
- Mathis, U. et al., Studies on the interactions of retinal dopamine with choroidal thickness in the chicken, Graefe’s Archive for Clinical and Experimental Ophthalmology (2023) 261:409–425
- Shu, Z. et al., The Role of Retinal Dopamine D1 Receptors in Ocular Growth and Myopia Development in Mice, The Journal of Neuroscience, 2023, 43(48):8231–8242
- Xiao, Q. et al., An Evidence-Based Narrative Review of Scleral Hypoxia Theory in Myopia: From Mechanisms to Treatments. Int. J. Mol. Sci. 2025, 26, 332.
- Yin, X. et al., The Role of Scleral Changes in the Progression of Myopia: A Review and Future Directions, Clinical Ophthalmology 2025:19 1699–1707
- Baksh, J. et al., Myopia Is an Ischemic Eye Condition: A Review from the Perspective of Choroidal Blood Flow. J. Clin. Med. 2024, 13, 2777.
- Sekaran, S. et al., Nitric oxide release is induced by dopamine during illumination of the carp retina: serial neurochemical control of light adaptation, Eur J. Neurosci. 2005; 21(8):2199-208.
- Perez-Fernandez, V. et al., Rod Photoreceptor Activation Alone Defines the Release of Dopamine in the Retina, 2019, Current Biology 29, 763–774, 2019.
- Liu, A-L. et al., The role of ipRGCs in ocular growth and myopia development, Sci. Adv. 8, eabm9027 (2022) 8
- Chakraborty, R. et al., Melanopsin modulates refractive development and myopia, Experimental Eye Research, 214, 2022, 108866
- Yang, Y. et al., Synergistic effect of defocus incorporated multiple segment glasses and repeated low level red light therapy against myopia progression, Scientific Reports, (2025) 15:3996
- Xiong, R. et al., Myopia Control Effect of Repeated Low-Level Red-Light Therapy Combined with Orthokeratology, Ophthalmology 2024, Vol 131 (11), p1304-1313
- Hon, Y. et al. Effectiveness of bright light therapy and combination with myopic defocus for controlling myopic eye growth in schoolchildren: study protocol for a randomised controlled trial (phase 1). BMJ Open Ophthalmology 2025; 10:e002044.
- Chun, R. K. et al., Additive effects of narrowband light and optical defocus on chick eye growth and refraction, Eye and Vision (2023) 10:15
- Yang Y, Xiao Z, Ouyang J, Guo Y. Synergistic efficacy of orthokeratology and 0.01% atropine in controlling pediatric myopia progression: A retrospective analysis. J Investig Med. 2025; 00(0):1-10.
- Tan, Q. et al., Combined 0.01% atropine with orthokeratology in childhood myopia control (AOK) study: A 2-year randomized clinical trial. Cont Lens Anterior Eye. 2023; 46:101723.
- Du, L. et al. Add-On Effect of 0.01% Atropine in Orthokeratology Wearers for Myopia Control in Children: A 2-Year Retrospective Study. Ophthalmol Ther. 2023; 12:2557–68.
- Wen, L. et al. Add-on effect of using 0.05% atropine in fast progressors of orthokeratology: A preliminary retrospective study. Cont Lens Anterior Eye. 2025; 48:102282.
- Erdinest, N. et al., Low-Concentration Atropine Monotherapy vs. Combined with MiSight 1 Day Contact Lenses for Myopia Management. Vision (Basel). 2022, 12;6(4):73
- Yum, H.R. et al., Synergistic Effect of Dual-Focus Soft Contact Lenses and 0.05% Atropine on Myopia Control in Children With Rapidly Progressing Myopia. Eye Contact Lens. 2025, 1;51(2):92–97.
- Guemes, V. N. et al., Defocus Incorporated Multiple Segments spectacle lenses and 0.025% atropine for myopia control in European children: 12-month results of a randomized clinical trial. 2024. Abstract presented at the International Myopia Conference in Sanya, China.
- Nucci, P. et al., A comparison of myopia control in European children and adolescents with defocus incorporated multiple segments (DIMS) spectacles, atropine, and combined DIMS/atropine. PLoS One. 2023; 18(2):e0281816.
- Cunha, C.M. et al. A real-world study comparing atropine monotherapy to the synergistic effects of combination treatment: Defocus Incorporated Multiple Segments spectacle lenses and low-dose atropine. 2024.
- Vagge, A. et al. Highly Aspherical Lenslet Target (HALT) technology in combination with low-dose atropine to control myopia progression. Invest Ophthalmol Vis Sci. 2024; 65:2739. Abstract presented at the 2024 ARVO Annual Meeting, Seattle, WA, 2024
- Jones, J.H. et al., Effect of Combining 0.01% Atropine with Soft Multifocal Contact Lenses on Myopia Progression in Children. Optom Vis Sci. 2022, 1;99(5):434-442.